There are many common beliefs about knee osteoarthritis that may affect your behavior and impact your rehabilitation. The purpose of this section is to address the most common misconceptions about knee osteoarthritis.
This is myth number one!
It is a common belief that the amount of degeneration seen on a scan (usually X-ray), is directly related to the amount of pain and disability a person has. Research suggests this isn’t the case!
Although structural changes may play a role, there are many other factors, some less obvious, which contribute to each persons experience with osteoarthritis.
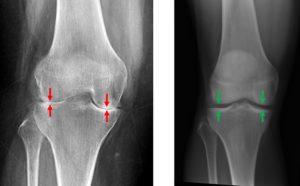
For example – you may have more pain and disability at your knee compared to Mr Smith (below).

However Mr Smith may demonstrate more degeneration (red arrows) in his Xray compared to your knee Xray (green arrows)
Read the rest of the myths about knee osteoarthritis and on the ‘what is osteoarthritis page’ to better understand causes of pain in osteoarthritis
Myth number two is that pain equals ‘damage’ or further degeneration – this is not the case.
Pain is very complicated and our knowledge and understanding of it continues to grow year on year. It is a common belief that if you have an increase in pain that you are damaging your knee structures.
We know that there are many causes and factors that can make your pain and symptoms worse, including:
– Being overweight
– Muscle weakness
– Doing too much
– Fatigue and being inactive
– Poor sleep
– Stress, depression, and feeling isolated
– Fear of damage and lack of joint confidence
– Other negative beliefs and mood
Fortunately, many of these factors can be changed or modified with appropriate guidance and support.
![]()
Read the rest of the myths about knee osteoarthritis and the ‘core treatments pages’ to better understand how you can manage some of these factors
Exercise is in fact very good for your knee osteoarthritis and is recommended as a safe and effective treatment for all persons with knee osteoarthritis.

Not everybody with knee osteoarthritis will be able to exercise to the same extent. What is important is that you get into a regular routine. You can get some examples of exercises from the ‘core treatment exercise’ section of this website.
Remember to be patient with your exercises and progress slowly over time – changes don’t happen overnight.

Read the rest of the myths about knee osteoarthritis and the ‘core treatments pages’ to better understand how you can more effectively plan and manage your exercising.
Rest used to be prescribed lots in the past for knee pains, however in most instances, rest and avoidance of exercise makes pain worse – especially in the long term.

As mentioned in myth 3 – we now know that exercise is actually very good for knee osteoarthritis. Therefore – it is important to ensure that you do not rely on rest and avoiding exercise/activities to help you manage your symptoms
Read the rest of the myths about knee osteoarthritis and the ‘core treatment education page’ to better understand how you can manage your pain.
No – this is not the case for the vast majority of people with knee osteoarthritis.
Guidelines suggest that surgery should be a last resort treatment for those who have not responded to PROLONGED and evidence based conservative management.
It is estimated that only 10-15% of those severe symptoms would be considered for surgery. Surgeries can include:
– Joint replacement (joint surfaces replaced with metal or plastic)
– Osteotomy
– Arthroscopic knee surgery
Food for thought:
Interestingly arthroscopic surgery has been found to have no better effect than a sham or placebo.
Additionally – a total knee replacement has no effect on pain levels in approx 20% of people.
Next – Treatments for knee osteoarthritis